
What is glue ear?
Glue ear is also known as otitis media with effusion (OME) which literally translates to ‘inflammation in the middle ear with fluid’. It is when the small middle ear cavity, usually filled with air, becomes full of a sticky fluid. The middle ear cavity contains the three tiny bones which pass on the sound vibrations from the eardrum to the cochlea. If this cavity fills with mucous (a bit like snot!), the bones don’t move as well, and this results in a hearing loss. To get a sense of the impact of glue ear, block your ears by pressing your fingers on your ears. The effect is very noticeable, particularly if you are trying to listen in a noisy environment, Glue ear is really common in children and by the age of 10, 80% of children will have experienced at least one episode of this.
Glue ear causes a conductive hearing loss of an average of around 30 decibels, although this can vary between children and typically also varies for the individual child. Often referred to as the ‘silent syndrome’ by health professionals, glue ear can have a significant impact on a child’s speech and language development and learning, if it persists for some time. Although usually a condition seen in children, adults can at times, experience episodes of glue ear.
How does glue ear occur?
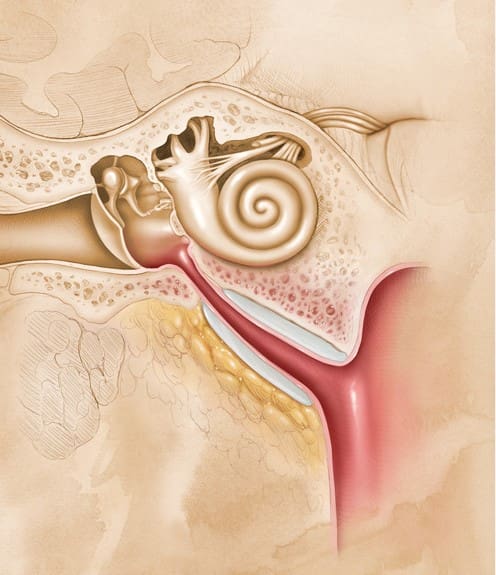
The middle ear space connects to the back of the throat/nose via the eustachian tube. Think of this tube as the link between the enclosed middle ear cavity and the outside world! When we swallow and yawn, the eustachian tube will open and close, thus keeping the air pressure in the middle ear space the same as the air pressure outside the head. This tube in fact helps us equalize pressure when say flying or diving. If this tube gets stuck and doesn’t open, often due to some inflammation, the air pressure in the middle ear drops (goes negative compared to outside air pressure) and eventually the cells in the middle ear start to produce a fluid/mucous.
Initially, this fluid is runny and will only minimally affect a person’s hearing. As more fluid is produced, the fluid gets thicker and stickier and will start to affect the hearing more. In children, the eustachian tube isn’t as vertical or wide as it is in adults, so it gets blocked more easily, and any resulting fluid in the middle ear doesn’t drain away as easily. If the fluid does manage to drain away through the eustachian tube, hearing usually returns to normal.
What causes glue ear?
Different things can contribute to the risk of a child getting glue ear. These include whether a child was breastfed, if a child has allergies, whether they are more prone to colds and infections. Some children who have lots of ear infections are more prone to glue ear, as are some children with cleft palate or Down’s syndrome. There is some evidence which links higher rates of glue ear if children are in smoky environments.
How would I know if my child has glue ear?
The most common signs of glue ear include the following:
- asking people to repeat what they say
- asking for the TV or music to be turned up loud
- struggling to hear people far away
- speaking loudly
- regression of speech and language becoming less
- become easily distracted when people are talking
These signs can often be mistaken for poor behaviour. As a result, many children with glue ear are misunderstood or labelled as ‘difficult’ or ‘naughty’. Glue ear can cause temporary hearing problem, and a prolonged period of time with reduced hearing can affect the way in which a child’s speech develops. For example, parts of words may not be pronounced clearly. However, evidence suggests that children catch up from any speech and language delay once they have recovered from glue ear.
It is also known that up to 80% of learning comes from incidental learning when children absorb sounds and other everyday input from their surroundings. Children with glue ear may thus fall behind at school and become disruptive if they don’t have extra support. It is crucial therefore for parents to be aware if their child is experiencing any impact from glue ear. Blog- Is my child hearing me?
What are treatment options?
A GP will examine your child’s ears and should be able to tell if they have glue ear. They may describe your child’s ear or ears as being ‘congested’. Your GP will often recommend pain relief if your child is complaining of painful ears. Antibiotics are not recommended for glue ear or for normal childhood ear infections, so your GP will only prescribe these if there are signs of a more serious condition.
Your GP can refer your child for a hearing assessment or you may request this yourself. Typically, an audiologist, specially trained to work with children will assess your child. They will assess your child’s level of hearing using age-appropriate techniques, as well as performing a tympanogram, which provides information about the middle ear and the function of the eustachian tube. Children’s hearing test.
If glue ear is found, for many children , there will be a period of ‘watchful waiting’ to see if it clears up by itself. This usually means a repeat hearing test after 3 months. If it doesn’t clear up or there are also concerns regarding a child’s tonsils, adenoids, speech and language development or other medical/developmental concerns, a referral to an Ear Nose and Throat (ENT) doctor is usually made.
Sometimes during this waiting phase, an otovent is recommended. Otovent is a device made up of a balloon and a nosepiece. The treatment involves fitting the balloon to the nosepiece, putting the nosepiece against one nostril, and keeping the other nostril and mouth closed, whilst attempting to inflate the balloon. It works by using pressure to open the eustachian tube, allowing the fluid to drain from the middle ear. This needs to be done daily for a set period and can be a bit tricky for young child to perform. For some children, there is evidence that this can help avoid surgery for glue ear.
Surgery, in the form of grommet insertion can be used for children where the fluid is not draining away by itself. Under a general anaesthetic, a small incision is made in the eardrum, fluid is then drained away from the middle ear and a tiny ventilation tube (grommet) is positioned in the eardrum to allow air to enter. Thus, if successful, hearing should return to normal levels, the middle ear is ventilated, even if the eustachian tube remains closed, and the child should experience good hearing and an absence of glue ear.
The surgeon may talk to you about removing your child’s adenoids at the same time. Adenoids are glands at the end of the eustachian tubes that sometimes become infected and swollen and block the end of the tubes.
Grommets usually stay in until the eardrum has healed and pushed them out, often 6 –18 months. Sometimes the fluid in the middle ear returns and another grommet operation may be considered.

Hearing devices/hearing aids can also be used quite successfully during periods of reduced hearing. Specifically, bonce conduction hearing aids used with soft bands (for example, Oticon Ponto) (see below)

or devices which attach to the skin with special patches (MED EL ADHEAR) (see below) can provide really good access to sounds. Parents often report immediate benefit when their child wears these type of devices.

Can my child fly with glue ear?
Parents often ask if they can take their child on a flight if they are known to have glue ear. In general, children with glue ear don’t experience problems flying. Sometimes a doctor may suggest not flying if they notice a particular problem with the ears.
If, however a child doesn’t have any fluid in the middle ears, but their eustachian tubes are not quite fully opening and closing, then this can cause some discomfort when taking off and, more commonly, when landing due to changes in the air pressure in the aircraft. Sometimes pain relief is required during a flight or decongestants prior to flying.
Eating and drinking during take-off and landing will encourage the eustachian tubes to open and prevent discomfort. There are also some special earplugs (available from pharmacies) which help to reduce discomfort from changes in air pressure. Flying with grommets is fine. The grommets prevent the discomfort caused by changes in cabin pressure, so your child should not experience any discomfort if the grommets are in place ans working (a quick check with our audiologist at The Hearing Space, in Leeds, can confirm this).
How can I support my child if they have glue ear?
It’s important that glue ear is identified as early as possible and that parents, carers and teachers understand how it can affect a child’s hearing.
To make listening easier for your child, you should:
- get your child’s attention before you start talking
- make sure you face your child as much as possible and keep eye contact
- check that background noise is kept to a minimum
- speak clearly, without shouting
Teachers should be made aware of audiological results and advice. It’s important that your child is able to sit near the teacher in the classroom, that they understand what is said, and that they feel comfortable asking for repetition when they do not hear.
For an initial chat regarding your child’s hearing or to book any hearing test in Leeds, contact ‘The Hearing Space’.
Tel: 0113 8730444 Mobile: 07999 738588 E:hello@thehearingspace.co.uk